
Clinicians call for BP-lowering therapies that also protect long-term cardiovascular health.

Across Korea and China, hypertension specialists emphasized that treatment must extend beyond achieving normal blood pressure levels to actively improving cardiovascular outcomes and protecting long-term organ function.
Hypertension is often managed with the goal of bringing blood pressure into a controlled range. However, even within those ranges, disease progression can cause damage to the heart, brain, retina, kidneys, and arterial vessels. Such injury can result in ischemic heart disease, heart failure, stroke, cardiovascular complications, and progressive renal decline—including end-stage kidney disease—underscoring the need for more comprehensive management strategies.
In line with this shift, the European Society of Cardiology (ESC) updated its 2024 hypertension guidelines, introducing more intensive BP targets and recommending earlier, cardioprotective interventions.
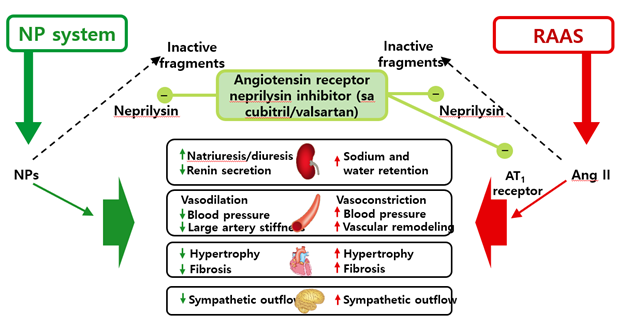
Among emerging therapeutic options, angiotensin receptor–neprilysin inhibitors (ARNIs) are gaining attention. Initially established as first-line therapy for heart failure, ARNIs act through a dual mechanism: enhancing protective natriuretic peptide (NP) pathways while inhibiting the renin–angiotensin–aldosterone system (RAAS).
In July, the ARNI Entresto (sacubitril/valsartan) received an expanded indication in Korea for hypertension. In response, the Korean Society of Hypertension held a dedicated session to review its clinical value in hypertension management.
Hit News spoke with Professor Wang Zhiguang, President of the Chinese Society of Hypertension and Head of Hypertension at Ruijin Hospital, Shanghai Jiao Tong University, and Professor Jin-ho Shin, President of the Korean Society of Hypertension and Internal Medicine Specialist at Hanyang University Hospital. The discussion covered unmet needs in hypertension care, the potential role of Entresto, and future directions for advancing treatment outcomes.

Entresto has now been approved for hypertension as well as heart failure. What changes do you expect in the treatment landscape?
Professor Shin: “From a therapeutic standpoint, I foresee two key changes. First, as heart failure treatments like ARNI have advanced, the traditional role of diuretics—such as SGLT-2 inhibitors—has been diminishing.
Second, most recent guidelines recommend using fixed-dose combinations with more than one pharmacologic mechanism as first-line therapy for hypertension, in order to improve both stability and efficiency of blood pressure control. Given that Entresto has long been used in heart failure due to its mechanisms—including natriuretic effects—it is likely to make meaningful contributions in hypertension, serving a preventive role at an upstream stage of the disease.”
What unmet needs exist with current hypertension therapies, and can Entresto help address them?

Professor Wang Zhiguang: “Traditional antihypertensive agents such as ACE inhibitors and ARBs have limitations in two key areas.
First, ACEis and ARBs do not provide sufficiently strong blood pressure–lowering effects. Second, while calcium channel blockers (CCBs) and diuretics can effectively reduce blood pressure, they are associated with more side effects. As a result, treatment guidelines generally recommend combining an ACEi or ARB with a CCB or diuretic to achieve adequate blood pressure control while protecting the vascular wall.
In contrast, ARNI therapy offers strong blood pressure reduction even as monotherapy, while also providing vascular and target organ protection. It can also be combined with a CCB or a thiazide (TZD) diuretic when needed.
The expanded indication for Entresto is meaningful because it allows us not only to control blood pressure more effectively, but also to simultaneously mitigate organ damage.”
How does Entresto work?
Professor Wang Zhiguang: “ARNI therapy has a very strong and well-defined mechanism for protecting blood vessels and organs. As Professor Shin mentioned earlier, when damage occurs in small or large vessels, ARNI can prevent this through its vasodilatory action. In the brain, for example, it can help prevent endothelial injury or arterial atherosclerosis.
In addition, the neprilysin-inhibiting component prevents the breakdown of natriuretic peptides such as ANP and BNP, thereby enhancing their effects. This promotes sodium excretion and reduces overall sodium retention. Since Asian populations generally consume more sodium than Western populations, this mechanism can be even more meaningful here.
ARNI also modulates the neurohormonal system by suppressing sympathetic activity and inhibiting aldosterone synthesis and secretion. By regulating neurohormonal pathways in this way, it supports overall vascular health and protects both small and large vessels. At the tissue level, it can also prevent fibrosis in the myocardium, vascular wall, and renal tissue.
In short, ARNI not only protects the vascular wall but also provides dual organ protection for the heart, brain, and kidneys.”
You highlighted organ-protection as a key advantage of Entresto. What mechanisms support this effect?

Professor Shin: “Hypertension causes persistent contraction of very small blood vessels, leading to structural changes and, as the condition progresses, fibrosis. These processes drive disease progression.
When systemic pathways such as the RAAS system are activated, this progression accelerates—directly damaging vessels or promoting fibrosis. Early on, these changes occur at the microvascular level and are usually not detectable clinically. As blood pressure rises further, larger vessels are affected, and the function of major organs—especially the brain and heart—can deteriorate rapidly.
Therefore, beyond lowering blood pressure, it is essential to prevent irreversible damage from the earliest stages. In this regard, drugs like ARNI, which can block multiple pathways of vascular and organ injury, are valued for their protective role and are expected to play an increasingly important part in treatment.”
Are there differences in how Korea, China, and Japan use Entresto?
Professor Wang Zhiguang: “Entresto was first approved in Europe for heart failure. Subsequent hypertension studies conducted in Asia demonstrated meaningful improvements, and China and Japan approved the hypertension indication earlier than Korea. However, the scope of use differs between the two countries.
In China, Entresto is used as a first-line therapy with the goal of effectively controlling hypertension. The 2024 Chinese hypertension guidelines now recommend ARNI as a first-choice agent.
In contrast, Japan still uses Entresto as a second-line option, typically in combination with a CCB or a thiazide diuretic. It is also used when ACE inhibitors or ARBs fail to achieve adequate control—mainly for refractory or difficult-to-manage hypertension.”
Professor Shin: “In Korea, the approval conditions are aligned with the hypertension trial design, meaning Entresto can be used in first-line patients. However, actual use depends on reimbursement criteria. How broadly it is adopted will depend on future discussions about cost-effectiveness. If this is resolved favorably, I believe Korea could use Entresto more widely than Japan.”
Among the hypertension studies on Entresto, which findings do you consider most notable?

Professor Wang Zhiguang: “Studies evaluating Entresto as monotherapy show that it delivers significantly stronger effects compared with traditional ARBs or ACE inhibitors. This is why, assuming equal pricing in China, ARNI has clear advantages and superiority.
The same holds true for combination therapy studies with Entresto and CCBs. If the price is equivalent, combining ARNI with a CCB is superior to using an ARB or ACEi first.
There have also been studies in special hypertension populations. For example, in treatment-resistant hypertension, the findings support using ARNI as a first-choice therapy rather than starting with an ARB or ACE inhibitor.
Although Entresto officially received approval as a hypertension treatment in China in 2021, it was already being used earlier for refractory hypertension. Beyond this, I believe ARNI therapy is essential for both treatment and prevention in patients with heart failure, chronic kidney disease, diabetes, coronary artery issues, or left ventricular hypertrophy—conditions where organ damage is a major concern.”
ARNI use is not yet recommended in Korean treatment guidelines.
Professor Shin: “Korea’s hypertension guidelines apply very strict criteria when designating a treatment as a Class 1A recommendation. I expect that most members of the guideline committee believe additional clinical evidence is needed before Entresto can receive a 1A grade.
However, speaking personally, considering the recommendation trends in other countries, it will be difficult for Korea to completely exclude ARNI. Rather than issuing a strong recommendation, I think it is more likely that ARNI will eventually be presented as one of the available treatment options.”
Which patients are most likely to benefit from ARNI?
Professor Wang Zhiguang: “First, ARNI should be recommended for patients whose blood pressure is not adequately controlled or who fail to reach target levels.
Second, I would recommend Entresto for patients with organ involvement—for example, those with proteinuria, advanced-stage kidney disease, or cardiac conditions that have progressed beyond left ventricular hypertrophy. Entresto not only lowers blood pressure but can also provide therapeutic benefit even when organ damage has already occurred, and in some cases may help reverse such damage.
In China, clinical studies and real-world cases have shown short-term improvement in patients with renal issues, such as proteinuria or declining kidney function, after initiating Entresto.”
Professor Shin: “ARNI is likely to provide the greatest benefit not to simple hypertension patients but to those with cardiovascular–kidney–metabolic (CKM) syndrome, in whom multiple systems are involved. This group is also the most likely to show clear differences between Entresto and other therapies.”
How do you expect the hypertension treatment landscape to evolve?
Professor Wang Zhiguang: “China alone has roughly 300 million hypertension patients, and worldwide the number reaches 1 billion. Managing and controlling blood pressure in such a large population is critically important. One approach, in my view, is to establish dedicated hypertension departments within medical schools to train more specialists capable of treating these patients.
Improving clinicians’ therapeutic capabilities is also essential—particularly in understanding which drugs can be used. Over the past five years, the introduction of ARNI marked an important beginning in China. Over the next decade, I expect many more drugs with novel mechanisms to emerge. If these are incorporated into new combination therapies, I believe we will be able to bring blood pressure within the normal range for a far greater number of patients.”
What efforts are needed to improve hypertension management in Korea?
Professor Shin: “Korea has one of the highest hypertension control rates globally, thanks to the dedication and efforts of our clinicians. Even so, we have now reached a saturation point—most issues that could be solved with traditional approaches have already been addressed.
The current challenge is how to better manage younger patients and high-risk groups. Hypertension in younger individuals is closely linked to obesity, while high-risk patients often have complex, treatment-resistant comorbidities.
For many years, our messaging around hypertension focused on severe outcomes: uncontrolled blood pressure could lead to death, disability from stroke, or suffering from myocardial infarction. But to the general public, these warnings may feel distant and abstract.
What we must emphasize now is that vascular and tissue damage occur continuously, even without symptoms, and that irreversible changes can develop quietly over time. It is crucial to communicate this clearly.
Clinicians should present hypertension management not as fear-based messaging but as a logical biological process, and offer concrete solutions—such as ARNI therapy or lifestyle interventions aimed at preventing tissue damage.
I believe that broader adoption of this kind of positive, constructive messaging will create an important breakthrough in improving hypertension control among Korean patients.”